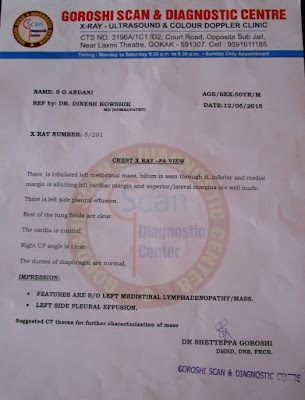
13-05-2015. Mr.S.G.A. aged 50yrs approached me with Chest pain and fever of 2 days duration. Patient was unable to give any significant history except that he had taken treatment for a corn on the left foot some months ago. The pain was sore and continuous - no significant modality. X-ray chest revealed a large mediastinal mass in front of the cardiac shadow and L. pleural effusion. Blood tests showed: Hb 13.3gm%; WBC count- 18,110/cu.mm; Polymorphs 80%, Lymphocytes 18%, Eosinophils 2%. My presumption was `enlarged lymph nodes'. An appointment for C-T scan was taken for the next day and simillimum in 200th potency was given till then.

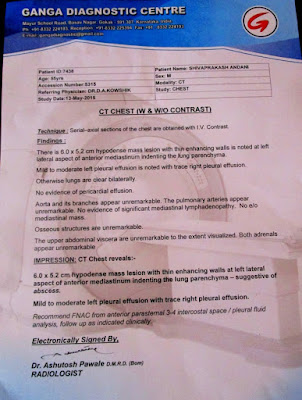
15-05-2015. CT scan reveals a huge (6.0X5.2 cms) mediastinal abscess with Left Pleural effusion. WBC total count 10,200/cu.mm; P 75%, L 22%, E 3%. The patient was having mild fever and chest pain persisted. Though the patient claimed that his chest pain had decreased I decided to continue the simillimum.
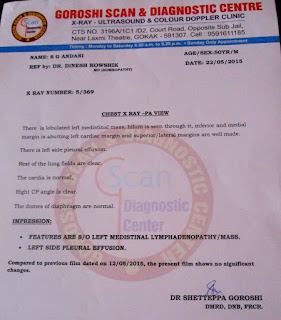
22-05-2015. X-ray chest shows no change in the mediastinal shadow. However patient was afebrile and did not complain of Chest pain.

25-05-2015. Patient has no complaints except a mild cough. O/E RS - Dullness in mediastinal region and L. lower chest with decreased air entry.
29-05-2015. Mild dry cough. No other complaints. O/E. RS - Air entry good on both sides. I now decided to give a deep acting remedy to complete the cure and remove the pathology.
18-06-2015. Patient has no complaints. X-ray shows remarkable improvement with reduction in density and size of the mediastinal shadow. Attached below are the series of X-rays, reports and CT scan report.


The First CT scan above shows a large grey rounded area Left and anteriorly which is the abscess. The grey semi-lunar area in the L. lower lung field is the pleural effusion.
The second CT scan taken 50 days later shows total resorption of the pleural effusion and only minimal traces of the abscess.

The patient is now on placebo and the follow-up continues.
ANALYSIS: Many a times we come up against pathological cases where the history is insignificant or unobtainable. This case despite being an acute case, had little to offer in terms of case history. I simply used common sense. The problem may have been caused primarily by inflamed lymphnodes in the mediastinum which later developed into an abscess. The rapid progress of this disease without any overt symptoms especially the minimal pain was remarkable. Belladonna being the primary prescription for acute inflamed lymph glands was ruled out due to the subdued symptom picture. The follow-up drug was chosen in 200th potency. Calc sulph was substituted for deep abscesses which helped further. A deep acting anti-psoric was then added to complete the cure. I do admit that this case leaves a lot of unanswered questions, but the point to be stressed is the ability of Homeopathy to treat such critical cases where investigations are the sole basis of the prescription, imbibing a bit of common sense to seek out the simillimum. As I have reiterated in my post on Acute cases, such life threatening cases with imminent death need quick thinking, good knowledge of MM and appropriate philosophy to be applied. Can Homeopathy treat all cases???????? The question begs an answer!
DISCLAIMER: This and any other article published here-with is not illustrative of a methodology and does not claim to advise anyone to attempt to handle such cases. Any such attempt to treat similar cases will be at the sole risk of the person attempting to do so. The author of this article will bear no responsibility for any mishap that may result from any attempt to treat critical cases based on any article published on this blog.

15-05-2015. CT scan reveals a huge (6.0X5.2 cms) mediastinal abscess with Left Pleural effusion. WBC total count 10,200/cu.mm; P 75%, L 22%, E 3%. The patient was having mild fever and chest pain persisted. Though the patient claimed that his chest pain had decreased I decided to continue the simillimum.

22-05-2015. X-ray chest shows no change in the mediastinal shadow. However patient was afebrile and did not complain of Chest pain.


25-05-2015. Patient has no complaints except a mild cough. O/E RS - Dullness in mediastinal region and L. lower chest with decreased air entry.
29-05-2015. Mild dry cough. No other complaints. O/E. RS - Air entry good on both sides. I now decided to give a deep acting remedy to complete the cure and remove the pathology.
18-06-2015. Patient has no complaints. X-ray shows remarkable improvement with reduction in density and size of the mediastinal shadow. Attached below are the series of X-rays, reports and CT scan report.

{kind=link}
{kind=link}


The First CT scan above shows a large grey rounded area Left and anteriorly which is the abscess. The grey semi-lunar area in the L. lower lung field is the pleural effusion.
The second CT scan taken 50 days later shows total resorption of the pleural effusion and only minimal traces of the abscess.

The patient is now on placebo and the follow-up continues.
ANALYSIS: Many a times we come up against pathological cases where the history is insignificant or unobtainable. This case despite being an acute case, had little to offer in terms of case history. I simply used common sense. The problem may have been caused primarily by inflamed lymphnodes in the mediastinum which later developed into an abscess. The rapid progress of this disease without any overt symptoms especially the minimal pain was remarkable. Belladonna being the primary prescription for acute inflamed lymph glands was ruled out due to the subdued symptom picture. The follow-up drug was chosen in 200th potency. Calc sulph was substituted for deep abscesses which helped further. A deep acting anti-psoric was then added to complete the cure. I do admit that this case leaves a lot of unanswered questions, but the point to be stressed is the ability of Homeopathy to treat such critical cases where investigations are the sole basis of the prescription, imbibing a bit of common sense to seek out the simillimum. As I have reiterated in my post on Acute cases, such life threatening cases with imminent death need quick thinking, good knowledge of MM and appropriate philosophy to be applied. Can Homeopathy treat all cases???????? The question begs an answer!
DISCLAIMER: This and any other article published here-with is not illustrative of a methodology and does not claim to advise anyone to attempt to handle such cases. Any such attempt to treat similar cases will be at the sole risk of the person attempting to do so. The author of this article will bear no responsibility for any mishap that may result from any attempt to treat critical cases based on any article published on this blog.